
Image Reference - https://images.pexels.com/photos/7578652/pexels-photo-7578652.jpeg?auto=compress&cs=tinysrgb&w=175&fit=crop&h=275&dpr=2
Generally, insightful visualizations express the hidden meaning within a given set of data. Data collected as healthcare indicators are no exception to this generalization. In this blogpost, an attempt is made to illustrate following two healthcare indicators by plotting in cartesian co-ordinates: -
Delivery Load per Facility – ‘Delivery Load per Facility’ to represent average number of deliveries per facility and be expressed as a “Decimal Number”. Delivery load may be calculated across a given geography for a given period of time (usually quarterly or yearly). If the delivery load is calculated from futuristic perspective, an estimated number of deliveries be calculated based on demographic and biological (like (say) fertility rate) considerations. If the delivery load is assessed for analysis of historical data, actual number of recorded deliveries be taken into consideration.
Per capita delivery load for Staff Nurse – ‘Per capita delivery load for Staff Nurse’ to represent average number of deliveries a single nurse has to attend and be expressed as a “Decimal Number”. Per capita delivery load for a staff nurse may be calculated across a given geography for a given period of time (usually quarterly or yearly). If the per capita delivery load is to be calculated from futuristic perspective, an estimated number of deliveries a nurse would have to attend is estimated based on historical data and based on predictive analysis of dynamics healthcare ecosystem. However, if the indicator is used for a period in the past, the actual recoded values of staff nurses be used.
Now, these indicators should include data from both public and private healthcare services. However, mostly, it is observed that such data are available only for public sector healthcare services. So for now, let us consider the above indicators to indicate public sector healthcare service provisioning.
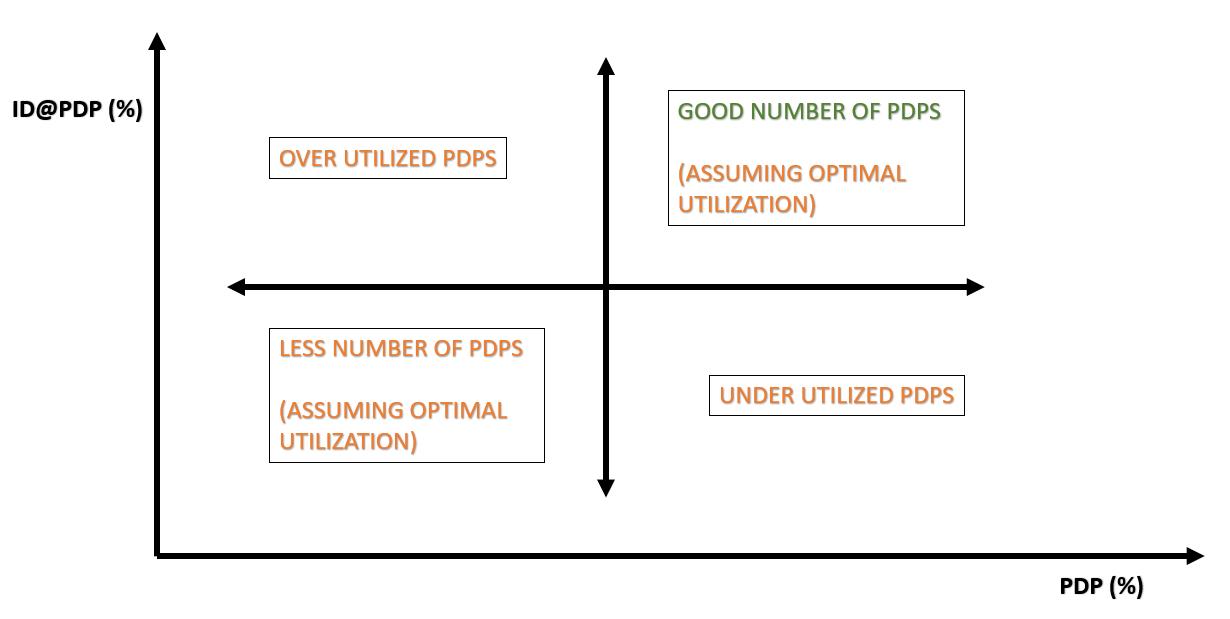
Keeping in mind the above discussions, let us attempt to show the above indicators in cartesian co-ordinates with Delivery Load per Facility in Y axis and Per Capita Delivery Load for Staff Nurse in X axis (refer to the graph is Figure - 1).

Figure – 1: Delivery Load per Facility versus Per Capita Load for Staff Nurse
It is evident from Figure – 1 that broad understanding on availability of staff nurses can be broadly assessed based on data visualization of the above mentioned two indicators. Assuming optimal utilization, the geographies with high Per Capita Delivery Load for Staff Nurses (average) and with high Delivery Load per Facility (average) could be considered to have good numbers of staff nurses and facilities may be getting utilized well. Similarly, assuming optimal utilization, the geographies with low Per Capita Delivery Load for Staff Nurses (average) and with low Delivery Load per Facility (average) could be considered under-utilized facilities. A low Delivery Load and high per Capita Deliver Load for Staff Nurse may indicate facilities with under-staffed nurses. And a high Delivery Load and low per Capita Deliver Load for Staff Nurse may indicate facilities with over staffed staff nurses.
However, while doing the above analysis (as depicted in Figure -1), the assumptions are as under: -
It is assumed that all other aspects influencing the above indicators remain unchanged.
All historical data are recorded accurately and future predictive analysis are reasonable.
Facilities are largely similar with nearly the same size and capacity, so that, averages taken into account hold reasonably well for analysis. RMNCH is dominant work carried out in public facilities with the assistance from ANM and GNM.
This is just to illustrate that a set of two chosen healthcare indicators may insist on resource utilization of healthcare facilities. When such an analysis is used, it is quite likely that within a significantly diverse geography and across a substantial period of time, the real data may fall in different ordinates of the cartesian shown above. In such a situation, meaningful inputs to healthcare management be given.
/**********************************/


{kind=link}